Rethinking the Health Paradigm
There must be a fundamental change from thinking of health as a cost to health as an investment. From ever more advanced treatment, the system must move to an ethic of prevention.
By Bogi Eliasen

Our health systems are under enormous pressure. There is constant increase in demand for access to treatment, in part, because the combined disease burden – the impact of a health problem as measured by financial cost, mortality, morbidity, or other indicators – is growing. There are several reasons for this. We have increased our lifespan over the last 150 years. We have also increased the average burden of disease. Thus the combined disease burden for the health system is ever greater.
In the Western world, communicable diseases have been substantially reduced: non-communicable diseases are the big challenges. These are largely caused by lifestyle and environmental factors. It is important to underscore that we will all die, and most of us from disease. The challenge we are facing is that we have a very high rate of avoidable disease burden that has a high cost for quality of life and dignity of the individual person, as well as health system resources.
But we have accepted as a law of nature that longer life spans have to come with increased disease burden. Why? We thus focus on very advanced treatments when people are already ill because we have both the knowledge and technology to assist and intervene. But for better impact we need to intervene as early as possible where disease can be cured or controlled at stages where the burden on the person is kept to a minimal level. We estimate that 30 percent of the current disease burden is avoidable. Our one-size-fits-all paradigm that has lifted our average lifespan from around 30 to around 80 has served us well, but is now outlived. We need a new way of thinking about health and sick care.
Dignity as a concept
To approach the question, we need to take a step out of the “factory” mindset in health. Health service provides people with better lives and requires a constant evaluation of what we do for the individual person. The core question is what we aim at: is it a better health system or a healthier population? This is not the same thing. We often forget that the most important attributes for our increased longevity are not our health systems, but factors like clean water, better and more education, improved housing, better work conditions, road safety, and less violence. There is a need to refocus on what keeps people healthier for longer, and where and how is it that we can help people the most. This includes rethinking what needs to happen in hospitals and what is better delivered outside the hospital.
Fourth industrial revolution
We are now witnessing the fourth industrial revolution in the field of heath: the combination of data, digital functions, new understanding of biology and biological tools, smart materials, and advanced used of imaging. We now work with data-driven health, real-time monitoring, genomics, and advanced imaging as a part of detection and treatments. We have experienced two decades focusing on precision medicine and health. The technology and knowledge is now ready to move to a more advanced stage. Precision is not just precision in the kind of treatment to provide, but also when to diagnose and when to intervene and follow up. The technology and knowledge at hand is currently held back by our separation of public and personalized health. These are two sides of the same coin where there is a need to rethink how we apply a concerted public and personalized approach to health at the same time. One of the core questions is: How do we apply resources where the impact is biggest?
Health as the most important societal pillar
In the data oversight we have in Denmark, there are clear patterns of disease trajectories that show both who is at high risk of chronic disease, but also at risk of other chronic diseases. Here it is important to have in mind that there is a substantial loss of quality of life for the patient with additional diseases, as well as complications in the health services. In the initiative Nordic Heath 2030, a collaboration across the Nordic countries started in 2019, one of the main conclusions is that health systems need to become much more preventive. Half of the health budget should have a preventive aim: primary, secondary, and tertiary prevention. This was based on a conclusion that we are not providing sufficient health outcomes for our budget and that the systems will break down if we do not change. It requires a fundamental change from thinking health as a cost to thinking health as an investment. There is also a need to identify the cost of inaction. While we have a technological explosion, we are lacking sufficient focus on capacity building on all levels to harvest the benefits of new technology and knowledge.
The change from life span to health span requires a hard change in thinking. We need to go from thinking about how long we live to how well we live. In the end, we will also increase longevity by focusing on how well we can live. Starting with secondary prevention makes sense. While general prevention is very important, our approach is to start with secondary prevention: working with the person at the earliest point of onset of a chronic disease or in high risk of chronic disease. This can only be done with a new way of thinking combining and connecting holistic and hyperspecialized mind sets. It is a new paradigm shift; we need to build new frames for technology and society.
Fairness, equity, equality justice
The building of a new health paradigm is dependent on technology, but we need to be very firm that technology is a tool, not the aim. We need to be very clear about what it is we aspire to, which is a healthier population, in which a better health system is one of the parts. But the aim is not the health system itself. The aim is to build a fairer, more equitable, and equal society that provides the opportunity for a healthy life leaving no one behind.
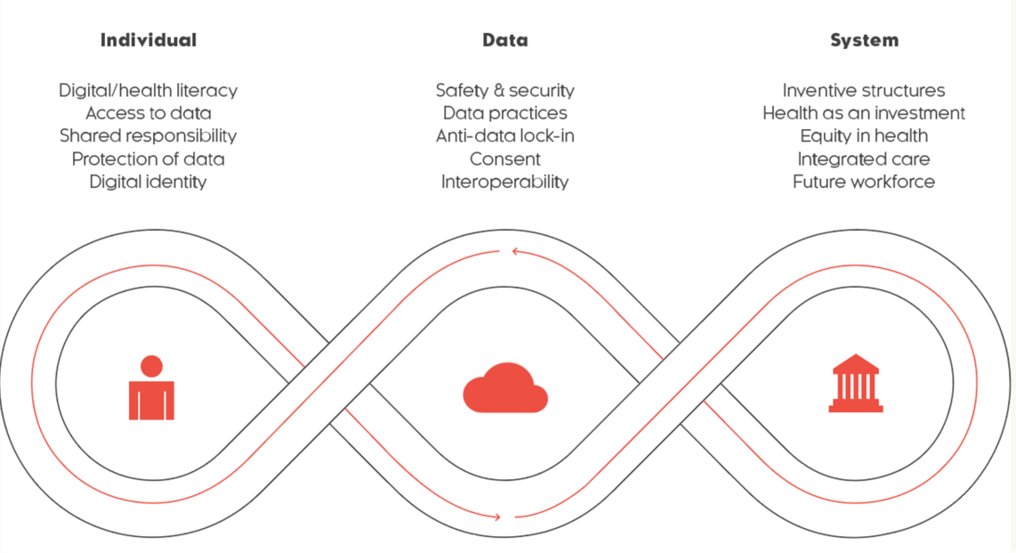
The intention behind publicly produced and/or funded data is crucial for establishing learning health systems. This doesn't just pertain to direct clinical health data, but also encompasses health-relevant data (any information pertinent to health/treatment and the like). Generally, this would involve aggregated data. Equally vital is the establishment of data intent at a personal level, ensuring that individuals always have access to linked data about themselves. This could pave the way for integrating both public and commercial data through a unified data intent strategy, as suggested by the World Bank.
The Humanome model is a product of the Nordic Health 2030 initiative launched in 2019, an endeavor led by the Copenhagen Institute for Futures Studies, in collaboration with the Nordic Councils organization, Nordic Innovation. This project was dedicated to fortifying cooperation in healthcare, with a spotlight on data, digital capabilities, and genomics. At its heart was empowering citizens by giving them access to their personal data. The goal was not just to provide data, but to ensure its relevance and value to individuals. Alongside this, the initiative prioritized the establishment of stringent safeguards and protocols uphold data security, individual autonomy, and contract compliance.
Data solidarity and no harm
The key question for data solidarity is whether a specific kind of data use is likely to create significant public value without posing undue risks. The Digital Transformation Health Lab headed by, among others, Ilona Kickbuch and Barbara Praisack proposes the establishment of a harm mitigation body that helps with data governance. This approach is very cautious in enabling responsible data use, not stopping it.
We are on the cusp of opportunities – and challenges – that can be a giant leap forward, or an unprecedented setback. We need to ask questions before seeking the answers if we want to address the new opportunities, challenges, and frames. If we only seek answers, we remain inside the current framework. The task ahead is not about advancing technology but about building a resilient and sustainable mindset and a new paradigm where we apply what we have.

Bogi Eliasen is Director of Health at the Copenhagen Institute for Futures Studies andRichard von Weizsäcker of the Robert Bosch Academy.